Medicine, post-racial America
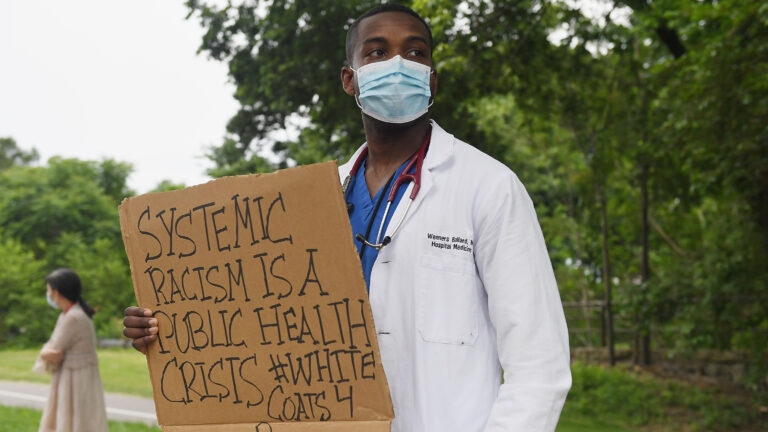
Silencing conversations about systemic racism in health care and the health care workforce prevents us from making progress.
A 2019 study analyzed 10 health care professions and found that Black, Hispanic and Native American people were underrepresented.
By Nazarul Islam
Do we recognize that Medicine has a race problem? And to add more fuel, there is a greater problem of people, talking about this race problem. Silencing conversations about systemic racism in health care and the health care workforce prevents us from making progress, and a large section of patients, who constitute the Black people or the people of color….are the ones who lose out.
It is not surprising that earlier in this month, the Accreditation Council for Graduate Medical Education (ACGME) placed Tulane University on probation amidst allegations of racism and sexism. In February, Tulane fired the residency director after she alleged the university had encouraged a culture of discrimination. After being made the director of another program, she sued Tulane, citing several challenges in carrying out her duties.
The editor of the prestigious Journal of the American Medical Association (JAMA) stepped down after asserting on a podcast that socioeconomic factors impacted health disparities, rather than racism. Of note, none of the experts on the panel were underrepresented minority researchers.
These events and others like them highlight a genuine concern. Are Americans ready to declare a post-racial America in medicine?
Two decades ago, American Institute of Medicine had released a landmark study that found racial disparities existed even when controlling for socioeconomic factors and factors such as geography and location of care. Blacks in academic medicine have been exposed to these disparities first-hand. They have received and continue to receive unequal treatment across the spectrum of medical care, varying from the inequitable receipt of pain medication to interventions for emergency cardiac care.
Obviously, there is some evidence that underrepresented minority patients do better in racially concordant relationships, highlighting the need for medical schools and residency programs to train more physicians of color. However, the number of underrepresented minority matriculants to U.S. medical schools is still well below what we would need to make real strides toward more equitable patient care.
To begin, a major issue is that medical education and medicine as a field already boast multiple barriers to entry for people of color. Historical factors from a not-so-distant era have contributed to an inadequate pipeline of Black physician trainees. Students of color often lack the encouragement needed to enter health care professions training and, in many cases, are actively discouraged.
Obviously, as the young physicians, residents in training often face micro aggressions from colleagues and stereotypes from patients. In a 2018 study published in JAMA, underrepresented minority medical residents reported frequent experiences of stereotypes from patients, colleagues and educators. Residents reported being referred to as members of the janitorial staff or asked about their country of origin.
America’s Residencies are perhaps doing a poor job in addressing these micro aggressions and biases, providing few opportunities to educate residents about race. Moreover, students often lack exposure to faculty role models. Only 3.6 percent of medical school faculty are Black, and only 5.5 percent are Hispanic. Of these, the majority are at the assistant level, with few holding faculty leadership positions.
Not surprisingly, Faculty and would-be administrators of color are met with resistance in their employment searches; and, when they do arrive on campus, they are met with isolation, skepticism, or total indifference towards their experience. Opportunities for growth and promotion are often stifled.
Again, the lack of diversity in medicine and health care is indicative of greater issues. Within health professions, training programs across the country exists a culture that fails to acknowledge and act on the criticisms presented by the unheard. It would be disingenuous to expect that the lived experiences of Black people and people of color suddenly matter in clinics and classrooms when they are routinely minimized across society.
The status quo prevails as Americans manage to tiptoe around racism with language such as “disparities, cultural competency or social inequities” to avoid uncomfortable discussions about the issue. Each of these topics is important, but none of them is a substitute for the very real conversation that we need to have about race and its role in medicine.
Silencing accusations of racism rather than engaging with them productively is a major impediment to meaningful progress. True change to the power structures that generate the injustice in medicine will require systems of accountability to be firmly in place. Protecting those who come forward and holding injustice accountable will not only help break that silence, but it will also create space for Black people and people of color in our field to speak openly about the changes we must make to our systems to advance racial equity in medicine.
Many in the industry do applaud that the JAMA and ACGME are making institutions and individuals accountable, but we must take the next step. We need more diversity in the health care workforce, and to increase diversity, we need to improve access to medical training.
A 2019 study analyzed 10 health care professions and found that Black, Hispanic and Native American people were underrepresented. This lack of representation persists in the health care training pipeline. We have mapped out the scale of the problem. Now, we need to identify and reduce the barriers to entry facing underrepresented minority youth, and we need to do it systematically across the entire health care workforce.
Systemic racism impacts every sector of society, and medicine is not immune. If we fail to talk about it honestly, we cannot make progress, and our patients lose out on better, more equitable care. We must improve the medical pipeline to help create a diverse workforce, and we must promote an environment where opinions about race and grievances can be heard.
Let’s not forget: More silence just means more of the same.
(Research: JAMA)